

Background: Peripheral T cell lymphoma (PTCL) is a heterogeneous group of aggressive lymphoid neoplasms with poor outcomes. Many patients are elderly with increased comorbidities. Single-center retrospective studies describe outcomes in elderly PTCL patients and suggest comorbidity adversely affects outcomes. Little is known about the treatment, outcomes and impact of comorbidity in a large cohort of elderly PTCL patients. This study aims to describe outcomes of elderly PTCL patients in a large unselected international patient cohort.
Methods: Patients with PTCL age ≥ 70 diagnosed from January 1, 2010 - December 31, 2015 in the Swedish Lymphoma Registry (SLR) and California Cancer Registry (CCR) were identified. The SLR covers ~ 95% of adult lymphoma patients in Sweden and the CCR includes information on all cancers diagnosed in California. Patients with precursor T-cell malignancies, primary cutaneous lymphomas, and leukemic subtypes were excluded. Data on comorbidity at diagnosis were retrospectively collected according to the Charlson Comorbidity Index (CCI) and clinical outcomes of the cohort were extracted.
Statistical analysis: Patient characteristics, clinical variables and outcomes were summarized using descriptive statistics and compared by Chi-square or Fisher's exact test. Outcomes of interest included overall survival (OS) and cause of death. Kaplan-Meier estimates of OS stratified by groups were calculated and presented in figures. Median OS was reported with 95% confidence interval (CI). Comparisons between groups for OS were done by log-rank test. Univariate and multiple Cox proportional hazards models provided hazards ratio estimates and 95% CI for risk factors. Tests for significance were two-tailed and a p-value less than the 0.05 significance level was considered statistically significant. Analyses were performed using software SAS version 9.4 (2013).
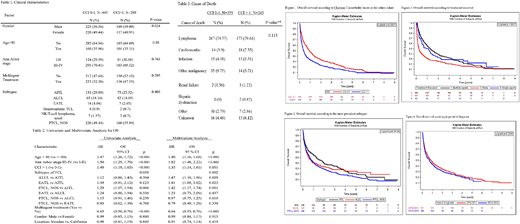
Results: A total of 839 patients were included (SLR, n = 176, CCR, n = 663). Median age was 78 (SLR) and 79 (CCR) years, respectively. Included subtypes were AITL, n = 226; ALCL, n = 122; EATL, n = 31; Hepatosplenic TCL, n = 7; NK/T-cell lymphoma, n = 10; and PTCL NOS, n = 443. ECOG performance status was not available. CCI data was available in 731 patients (87 %), and CCI scores were divided into groups = 0-1 (61 %) and CCI > 1 (39 %). Male patients more often had a CCI score > 1 (p = 0.024). No other significant baseline differences were seen between the 2 groups (Table 1).
Patients in the SLR more often received multiagent treatment compared to the CCR (63 % vs 44 %, p < 0.001). Age > 80 years, CCI > 1 and advanced Ann Arbor stage (III-IV) were significant prognostic factors for worse outcome. No difference in survival was seen between men and women nor the SLR and CCR (Table 2).
Patients with a CCI >1 had a statistically significant worse survival compared to patients with a CCI =0-1 (0.36 years v 0.91 years, p=0.0001). Of the PTCL subtypes, AITL patients had a significantly better outcome (median OS = 1.26 years) compared to ALCL (OS = 0.57 years) and PTCL NOS (OS = 0.66 years). Patients receiving multiagent therapy had improved survival compared to patients not receiving multiagent therapy. When comparing OS in patients diagnosed in 2010-2012 with 2013-2015, no improvement was seen for the later period (Figures 1-4).
Lymphoma was the most common cause of death with > 70 % of deaths related to lymphoma irrespective of CCI score (Table 3).
Discussion: At the time of submission, this study presents the largest international cohort of elderly patients with PTCL. Prognosis is poor and comorbidity seems to further worsen . In contrast to younger patient series, patients with AITL had a better survival than patients with PTCL NOS and ALCL, and were more common in the CCR than in the SLR. Multiagent treatment was associated with improved outcome. A possible confounder could be that fit patients are also the ones receiving treatment, and it is a setback that adjustment for ECOG was not possible, making treatment data somewhat difficult to interpret. As expected, advanced stage (Ann Arbor III-IV) was associated with worse survival.
Conclusion: We believe this is one of the largest cohorts presented in elderly patients with PTCL. Comorbidity is an important adverse factor in this group, whereas treatment seems to improve outcome. The majority of these patients die of lymphoma within a year from diagnosis, and development of new treatments represents an unmet clinical need.
Jerkeman:Abbvie: Research Funding; Gilead: Research Funding; Celgene: Research Funding; Janssen: Research Funding; Roche: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal